
Your Fertility Test Results Explained: What’s “Normal” vs. Not (and What to Do Next)
Getting fertility test results can feel like getting a report card—especially when the numbers are unfamiliar and Google makes everything sound urgent. Take a deep breath: most fertility results are not “good” or “bad.” They’re clues your care team uses to understand what might be affecting conception and what treatment path makes the most sense.
This guide explains the most common fertility tests, what they measure, what results are often considered typical, and—most importantly—what your numbers can and cannot tell you.
Important note: “Normal” ranges vary by lab, testing platform, and clinical context. The examples below are for education and should be interpreted with your provider using your lab’s reference ranges.
The Big Picture: What Fertility Tests Are Really Designed to Do
A fertility evaluation is less about predicting whether you’ll get pregnant and more about answering questions like:
-
Are you ovulating regularly?
-
Do your ovaries look like they’ll respond well to fertility medications?
-
Is sperm count/movement within expected ranges?
-
Are the uterus and fallopian tubes healthy?
-
Are there hormone issues that could interfere with ovulation or implantation?
Some tests assess egg quantity (ovarian reserve). Others assess timing, ovulation, anatomy, or sperm factors.
One key concept to remember: “Normal” ≠ “No fertility issue.”
You can have normal test results and still face infertility (for example, unexplained infertility). That’s why tests are interpreted together, not in isolation.
Ovarian Reserve Testing: Egg Quantity (Not Egg Quality)
Ovarian reserve tests roughly estimate how many eggs may be available and how you might respond to ovarian stimulation medications—especially for IVF or egg freezing. However, major reproductive societies emphasize that ovarian reserve markers are better at predicting egg yield than predicting pregnancy on their own, and should be interpreted alongside age and clinical context.
1) AMH (Anti-Müllerian Hormone)
What it is: A blood test that reflects the overall activity of small follicles in the ovaries.
What it’s used for: Estimating ovarian reserve and predicting how you might respond to ovarian stimulation; it’s not a standalone predictor of your ability to conceive.
Common interpretation (high-level):
-
Lower AMH may suggest fewer recruitable follicles (potentially lower response to stimulation).
-
Higher AMH may suggest more recruitable follicles (sometimes seen in PCOS).
Why numbers are tricky: AMH values vary by age and by lab assay; interpretation should be individualized, and AMH is not a direct measure of egg quality.
2) AFC (Antral Follicle Count)
What it is: A transvaginal ultrasound count of small resting follicles, typically performed early in the cycle.
What it’s used for: Along with AMH, AFC helps estimate ovarian reserve and guide medication dosing in IVF and egg freezing discussions.
Common “typical” range you may see discussed: Many fertility education resources describe an AFC around 10–20 total follicles (both ovaries) as a common “normal” range, with lower counts potentially suggesting lower reserve.
What AFC can’t tell you: AFC reflects quantity, not egg quality, and results can vary by cycle timing and ultrasound technique. Importantly, AFC does NOT predict fertility.
3) Day 3 FSH and Estradiol (E2)
These labs are often drawn on cycle day 2–4 to capture a baseline.
Day 3 FSH (Follicle Stimulating Hormone)
What it is: A pituitary hormone that signals the ovaries to recruit follicles.
How it’s commonly framed:
-
Day 3 FSH < 10 IU/mL is often cited as a typical normal baseline.
-
Higher values can suggest the brain is “pushing harder” to stimulate the ovaries, which can be associated with diminished ovarian reserve (DOR)—though interpretation depends on age and estradiol and the time in cycle.
Day 3 Estradiol (E2)
What it is: A form of estrogen produced by developing follicles.
A commonly cited baseline: E2 < 50 pg/mL on day 3 is often referenced as typical.
Why FSH and E2 are paired: Estradiol can be elevated early in the cycle and “mask” FSH (making FSH look more normal). That’s why clinicians interpret these together
Male Fertility Testing: Semen Analysis (SA)
A semen analysis is one of the most informative and least invasive fertility tests. Results can fluctuate, so a single analysis is often not the full story.
Key semen analysis reference values (WHO 2021)
The World Health Organization (WHO) provides widely used reference values based on men whose partners conceived within 12 months.
WHO 2021 lower reference limits (5th centile) include:
-
Volume: 1.4 mL
-
Total sperm number: 39 million per ejaculate
-
Concentration: 16 million/mL
-
Total motility: 42%
-
Morphology (normal forms): 4%
What “below range” can mean:
-
Sometimes it’s a transient factor (e.g., illness, heat exposure, medication, time since last ejaculation)
-
Sometimes it points to a treatable medical or lifestyle contributor
-
Sometimes it changes which fertility options are most effective (e.g., IUI vs. IVF vs. IVF with ICSI)
What “normal” can’t guarantee: Even normal parameters don’t always rule out male factor issues; results are interpreted alongside history and sometimes additional testing.
Thyroid (TSH): A Common “Supportive” Test
Thyroid health can influence ovulation and early pregnancy. In fertility care, you’ll often see clinicians aiming for tighter TSH control than what’s considered “normal” for the general population.
Why TSH targets differ when trying to conceive
The American Society for Reproductive Medicine (ASRM) notes ongoing debate in how subclinical hypothyroidism is defined and managed in infertility, and that professional recommendations vary; it’s an area where individualized guidance is important.
A commonly used goal: Current guidelines and clinical practices aim for TSH < 4.0 mIU/L during preconception and early pregnancy planning—especially for patients with known hypothyroidism.
Imaging Tests: “Numbers” Matter Less Than Findings
Some of the most important fertility evaluation results aren’t numeric—they’re based on whether structures look normal.
HSG (Hysterosalpingogram) / SIS (Saline Infusion Sonogram)
These tests evaluate:
-
Whether fallopian tubes appear open
-
Whether the uterine cavity has findings like polyps, fibroids, scar tissue, or abnormal shape
If your report uses terms like “patent tube,” “filling defect,” or “hydrosalpinx,” your care team will explain what it means for next steps.
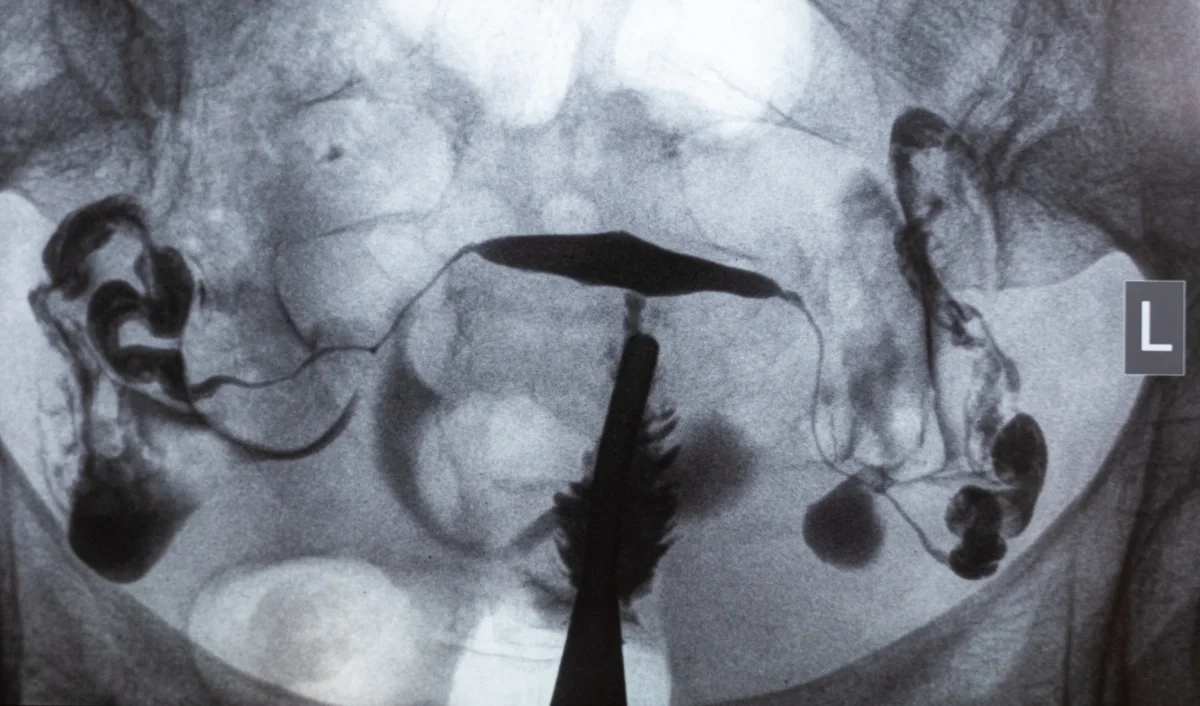
X-ray image of an HSG
A “Before You Panic” Checklist (Please Read This)
If you take nothing else from this blog, take this:
1) One number rarely tells the story.
Ovarian reserve markers are helpful for planning, but reproductive societies emphasize they are limited as stand-alone predictors and should be interpreted with age and clinical context.
2) “Abnormal” does not mean “no options.”
Many people with low ovarian reserve still conceive—sometimes naturally, often with tailored treatment strategies.
3) “Normal” does not mean “nothing is wrong.”
That’s why “unexplained infertility” exists, and why treatment can still help even when testing looks okay.
4) Your lab’s reference ranges matter.
Different platforms and labs can report different ranges—especially for hormone assays.
What Happens Next? How Fertility Specialists Use Your Results
Rather than “grading” your fertility, your care team uses results to personalize:
-
Whether starting with timed intercourse, ovulation induction, IUI, or IVF makes sense
-
How time-sensitive your plan may be
-
Medication dosing and monitoring
-
Whether additional testing is needed (genetic screening, uterine evaluation, male-factor workup, etc.)
When Should You Talk to a Specialist?
Consider scheduling a consultation if:
-
You’re under 35 and have been trying for 12 or more months
-
You’re 35+ and have been trying for 6 or more months
-
You have irregular periods, known endometriosis/PCOS, recurrent pregnancy loss, or male-factor concerns
-
You’re considering egg freezing and want a personalized plan
Final Thought: Your Results Are Information—Not a Verdict
It’s completely normal to feel overwhelmed by fertility testing. But your numbers are not your future. They’re a starting point for a plan—one that should be tailored to your goals, your timeline, and your full clinical picture.
Ready to Review Your Results Together?
Fertility test results can bring up a lot of questions—and you don’t have to sort through them alone. At Advanced Fertility Center of Chicago, our physicians take the time to review your results in context, explain what they mean for you, and walk you through your options with clarity and compassion.
Whether you’re just starting out or deciding on next steps, we’re here to help you feel informed and supported. Schedule your fertility consultation today.
Categories
About the AFCC Blog
Welcome to the Advanced Fertility Center of Chicago’s blog! Here, you will find information on the latest advancements in fertility care and treatments, including IVF, IUI, third-party reproduction, LGBTQ+ family building, preimplantation genetic testing, and more. Since 1997, we’ve used our experience and continuous investment in the latest fertility technology to help thousands of patients grow their families. Contact us today for more information or to schedule a new patient appointment.